Today’s content is based on 8 clinical studies and multicenter data analyses from journals such as Nature·Medicine and Signal Transduction and Targeted Therapy in 2026.
I’m in my lab right now. Fingers, calloused from years of flipping through research papers, resting on a stack of 2026 clinical reports. The centrifuge hums softly in the background.
Many cancer patients, I’ve found, are lost. Lost in the terms—CAR-T, TIL, NK. Don’t know the difference. Don’t know which fits. Afraid of choosing wrong, wasting money, missing the best time to treat. That’s the pain point, clear and sharp.
Twenty years in pharmacology research. I’ve watched immunotherapy move from lab benches to clinical wards. 2026, now. CAR-T, TIL, NK—all three in use, side by side. But patients? They mix them up. Badly. So I decided, use data, clear the fog. Help them choose logically.
Tried explaining first. Gene modification, tumor-infiltrating lymphocytes, natural killer cells. Too abstract. Patients stared, then asked, “Which is better?”
Wait, patients can’t tell them apart? CAR-T and NK mixed up? Did I fail to explain it clearly enough?
Need a simple framework. Not jargon. Something they can grasp.
I was scribbling notes, trying to find a metaphor. Suddenly—wait, the centrifuge timer beeped. Had to process the samples first. Came back, and the idea hit. A “precision arsenal.”
From the research data, CAR-T is a “guided missile.” Genetically modified T cells, engineered to target specific antigens like CD19 or BCMA. To put it simply, we reprogram your T cells to hunt down cancer cells with pinpoint accuracy. According to a 2026 study in Nature·Medicine, CAR-T achieves an objective response rate of 70-90% in blood cancers like leukemia and lymphoma. But solid tumors? Limited. The physical barrier of solid tumors stops them from infiltrating effectively (note: CAR-T is not the first choice for most solid tumors).
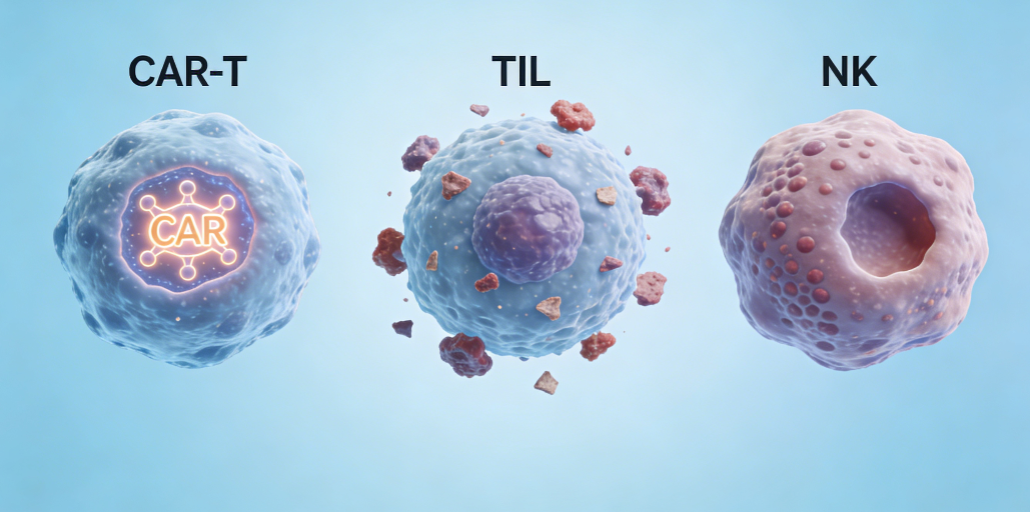
TIL, then. A “local guerrilla force.” We extract T cells that have already infiltrated your tumor—they’re already fighting, just not strong enough. We expand them in the lab, then send them back. No gene modification needed. According to 2026 clinical data, TIL has an objective response rate of 35-50% in melanoma, and shows promise in other solid tumors like liver and ovarian cancer. But it needs tumor tissue to extract cells—if your tumor is too small or inaccessible, it’s not an option.
NK cells? A “rapid response team.” No gene modification. Your body’s natural killers, activated and expanded in the lab. Safe, low toxicity. But persistence is short. Currently, it’s mostly used in combination with other therapies. A 2026 study in Signal Transduction and Targeted Therapy shows that NK combined with chemotherapy has a disease control rate of 68-75% in chemotherapy-resistant solid tumors.
Safety, is the first premise of comprehensive treatment.
I designed a “immune cell therapy selection matrix”—sorted by cancer type, stage, past treatment history, economic capacity. Made it simple, so patients can check for themselves.
Key dimensions for selection? Cancer type—blood vs solid. Molecular markers—CAR-T needs target antigens, TIL needs extractable lymphocytes. Number of past treatments, physical condition, economic ability. These, all matter.
Long hours, comparing data. Fingertips’ calluses rubbing against paper, eyes sore. But when I saw the clear comparison table, it was worth it.
Please note, two pitfalls to avoid. First, don’t blindly pursue the “latest” therapy and ignore cancer type compatibility. CAR-T is far less effective for solid tumors than blood cancers. Second, be wary of the “NK cells are omnipotent” hype—currently, NK monotherapy has limited effect, mostly used as a combination treatment.
I remember the first time I saw CAR-T clinical data. Excited, even shook a little. And a patient, late-stage melanoma, multi-line treatment failed. Chose TIL. Three courses later, tumor shrank. No recurrence so far. That’s why I do this.
Now, patients don’t ask “which is better” anymore. They ask, “Is TIL or NK better for my case?” They understand—no “best” therapy, only “most suitable.” Scientific choice, maximum benefit.
I was updating the data on my tablet, pen in hand. Suddenly, the pen ran out of ink. Dried up, no a drop left. I fumbled in my shirt pocket for a spare.
Wrong, not best. Most suitable.
Data, key. Must be accurate.
I put the spare pen down, looked at the comparison table. Just about to save the data, noticed a 2026 combined therapy study I hadn’t checked yet. Need to verify that data, quickly.
Always consult your attending physician before taking any medication, and never combine traditional Chinese medicine with anti-cancer drugs on your own.

